
Management of white spot lesions
Decalcification is the number 1 reason that orthodontic practitioners get sued. Therefore, preventing decalcification and white spot lesions is an important aspect of management of legal risks associated with orthodontic treatment. And even more important than the legal considerations are the aesthetic implications for your patients. Improving dento-facial aesthetics is one of the primary reasons that patients seek orthodontic care. Aesthetics are severely compromised when decalcification rears its ugly head. Prevention of these problems leads to better aesthetics and, as a result, more satisfied patients. In this post, I will discuss prevention and treatment of white spot lesions. Numerous links to articles and product information are included in the post. This gives you the opportunity to learn the best techniques for prevention and treatment of this problem.
Preventing decalcification
Nothing works better than good oral hygiene. Take the time to explain and show proper brushing techniques to your patients. At each monthly visit, carefully evaluate the patient's hygiene. Continually work with the patient on brushing technique, making sure the patient is aware of areas he or she may be missing when brushing. Nightly use of a fluoride mouth rinse has been shown to be very effective at preventing decalcification.
http://www.ncbi.nlm.nih.gov/pubmed/12917928
http://www.actfluoride.com/dental-professionals/act-total-care-64-oz-professional-use-dispenser/
Also, make sure the patient gets his or her teeth cleaned regularly. In my practice we schedule all orthodontic patients for prophys at 4 month intervals. This is slightly more expensive for the patient (most dental insurance covers prophylaxis at 6 month intervals, so 1 cleaning a year is usually not covered by dental insurance), but the benefits gained outweigh this small disadvantage. The method of choice for efficient cleaning of teeth with bonded and banded appliances is a prophy jet (see links below for more information).
http://www.dentsplymea.com/content/cavitron%C2%AE-prophy-jet%C2%AE
http://www.dentsply.com/media/345951/dual_select_80518__r9__0512_.pdf
Smooth surface sealants
These are a relatively new class of products; the results achieved in elimination of decalcification have been impressive. Smooth surface sealants can be applied to the whole facial (or buccal) surface of teeth after etching. After curing the sealant, use your preferred bracket adhesive as directed. Some clinicians prefer to place this material around the brackets after orthodontic bonding is completed. Both techniques work well.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3242403/
http://www.relianceorthodontics.com/store/product.php?productid=37
Instructions for Use of PRO SEAL® and L.E.D. PRO SEAL® (courtesy of Reliance Orthodontic Products)
1. APPLICATION: Dispense a drop or two of PRO SEAL® onto a mixing pad. With a brush, apply a thin uniform layer on the etched enamel surface. Stroke over with the same brush to ensure a thin layer and proper coverage. If not applied in a thin layer, LED PRO SEAL® may appear yellow.
If using original PRO SEAL®, cure each tooth for 20 seconds with any corded halogen, plasma or LED curing light (390 – 440 nM). If using L.E.D. PRO SEAL®, cure each tooth for 20 seconds with any corded halogen, plasma or LED curing light (440-480 nM). The material is compatible with the majority of orthodontic adhesives.
Note: In order for PRO SEAL® to remain on a normal tooth surface, it must be applied to properly conditioned, dry enamel. Atypical enamel should be first etched and then conditioned with multiple coats of Enhance™ Adhesion Booster or Assure® Universal Bonding Resin, then lightly dried before the PRO SEAL® is applied. In order for PRO SEAL® to completely cure, a proper intensity light must be used for the prescribed time at close range.
If PRO SEAL® is cured and saliva contamination occurs, the contaminated tooth can be cleaned by dabbing lightly with Enhance™ or Assure® Sealant and dried with air.
2. REMOVAL OF SEALANT RESIN: After the adhesive paste has been removed with a Renew™ System Bur (#118S, #118L or #218), removal of PRO SEAL® sealant is easy. Use the #383 Renew™ System Point on your choice of handpiece. Lightly polish the entire tooth surface with the #383 rubber point where PRO SEAL® has been applied. Note: If patient will visit the hygienist during treatment, the enamel should not be cleaned with a prophy jet as this can remove the PRO SEAL®. Use fine pumice for cleaning.
A final note about prevention of decalcification
As dental practitioners, our most important duty when treating patients is to do no harm. Keeping this in mind, if, despite your best efforts, decalcification is occurring, the best thing to do is to stop the damage by removing the braces. In the great majority of cases, poor patient cooperation is the primary reason that decalcification occurs. Mouth rinses and sealants will often not prevent decalcification if the patient's hygiene is poor. In these cases (even though it may not seem like it at the time) the best thing you can do for the patient is to take the braces off. The teeth won't go away; orthodontic treatment may be re-initiated after hygiene improves. Following this advice will prevent a lot of problems. Logistically, early removal is a hard thing to do. Payment plans must be altered and it is not easy to convince a parent that this is the best course of action. But often it is the right thing to do, and waiting for a child to mature a little before re-treating will prevent a lot of future dental problems.
Management of white spot lesions
Despite our best efforts, decalcification does occur. It is never a good day at the office when white spot lesions are discovered when braces are removed. Fortunately, there are some new techniques that can be used to eliminate (or at least minimize) the size and scope of white spot lesions. The two best techniques are microabrasion and at home application of CPP-ACP.
Microabrasion is a technique where a combination of acid and pumice are used to remove enamel irregularities and discoloration defects. A step by step set of instructions as well as some case studies are presented in the article which can be accessed by using this link:
http://www.dentalaegis.com/cced/2011/04/smile-restoration-through-use-of-enamel-microbrasion-associated-with-tooth-bleaching
Studies show (see references in the article) that enamel microabrasion removes a "clinically insignificant" amount of enamel from the tooth surface. Additionally, the newly exposed enamel demonstrates a significant resistance to demineralization. For most patients 4 treatments done at 2 week intervals greatly reduce the size and discoloration of the lesions. For more information on this technique, go here http://www.youtube.com/watch?v=Zwkp5MBa9X8 and here http://www.dentalcare.com/en-US/dental-education/continuing-education/ce1004/ce1004.aspx?ModuleName=coursecontent&PartID=2&SectionID=-1
The second technique which can be used to eliminate white spot lesions involves the use of casein phosphopeptide amorphous calcium phosphate (CPP-ACP). The most widely used product is called MI Paste and is distributed by by GC America. For information about this product, follow this link http://www.breezecare.com/mediacenter/recaldent/orthomousseplus.pdf
MI Paste is intended for at home use. Patients apply the paste to the affected areas once a day for about a month. The material is rubbed on with either a q-tip or a finger tip. Lesion reduction is maximized if at each application the material is allowed to sit undisturbed for at least 3 minutes.
http://www.orthotechnology.com/product_literature/pdfs/B-MI_PREVENTATIVE.pdf
A final note
Many clinicians are reporting spectacular results in elimination of white spot lesions by using a combination of the two techniques. The Angle Orthodontist November 2012 issue contains an article describing how to combine these techniques. The article also reports results attained by doing this. You can access that article here: http://www.angle.org/doi/pdf/10.2319/090711.578.1
I strongly encourage you to read this article. It is very well written and provides a great summary of the methodology and potential results that can be obtained by using these techniques. You will benefit your patients by offering these services.
Friday, November 30, 2012
Sunday, May 20, 2012
Bracket repositioning
Question: In this treatment, initial leveling and aligning is complete, so it is time reposition the brackets. Here is the panorex. How do I know what brackets to reposition? Do I look at the way roots are supposed to be? In this case, no repositioning has been done; I just want to be certain I get the concept of repositioning brackets. Thanks for your time.

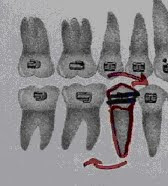
 Is there a method to quickly determine how to position brackets to achieve optimal root position? Fortunately, there is. Focus on the inclination of the bracket slot. If distal root movement is needed, angle the bracket slot disto-gingivally, and if mesial root movement is needed, angle the slot meso-gingivally. Look at the example below.
Is there a method to quickly determine how to position brackets to achieve optimal root position? Fortunately, there is. Focus on the inclination of the bracket slot. If distal root movement is needed, angle the bracket slot disto-gingivally, and if mesial root movement is needed, angle the slot meso-gingivally. Look at the example below.
 The outlined tooth (red) represents the current root position. To tip the root to the distal, change the inclination of the bracket slot so it is angled disto-gingivally.
The outlined tooth (red) represents the current root position. To tip the root to the distal, change the inclination of the bracket slot so it is angled disto-gingivally.


Right Left
Answer: Yes you do reposition brackets based on root position as viewed on on the panorex as well as (on premolars and molars) marginal ridge heights as viewed in the mouth. Ideal bracket positioning results in slight distal inclination of all the roots. In this case, I would reposition both upper lateral brackets because both roots are mesially inclined. By aligning the long axis of the bracket with the pulp canal (rotate both brackets disto-gingivally) distal root inclination will be accomplished. Also, the upper 1st premolar roots need more distal inclination and, on the lower, both lower 5's and the lower right 2 need more distal root inclination. After repositioning, use 016niti for a month to align the repositioned brackets. After aligning is accomplished, continue with mechanics. Here is a way to help position brackets correctly: At the repositioning appointment, take a panorex to check for incorrectly positioned brackets. Evaluate root position (also called 2nd order position), and reposition the brackets to improve root position. Also check posterior marginal ridge height and reposition brackets to obtain level marginal ridges. Repositioning is time consuming and difficult, but correcting 2nd order inclination will result in much better occlusion. Root inclination is the main focus of repositioning because 2nd order arch wire bends are difficult to make. When repositioning, first identify teeth with incorrect root inclination. Reposition the brackets on those teeth so the long axis of the bracket is parallel to the pulp canal. Ideally, brackets should be checked (and repositioned, if necessary) twice during treatment. The first repositioning is done after the wire progression is complete (usually about 7 to 10 months into treatment) and the second repositioning is done at the start of finishing (usually about 4 months before removal). Look at the x-ray below and evaluate root position. 


Here is how a correctly positioned
bracket should look.


Notice how changing the slot inclination changes how the root will be positioned. (Thanks to Gerry Samson, for allowing the use of these photos. You can find more information about Gerry’s CE courses at www.gnathosce.com .
Saturday, March 3, 2012
More Questions and Answers

I have a concern about this case. She has 016 nitinol in both upper and lower arches. Her right side looks good. My question involves the slight open bite on the right side. When and how should I correct it? Should I wait until I get to a stiffer rectangular wire, then use elastics?
There are two reasons why the bite is open in the canine area. First, the wire is not completely unloaded. It needs more time to totally straighten. In other words, if you look at the shape of the wire between the lateral and 1st bi, it is not straight, but still slightly rounded. It will be straighter after another 4 weeks, so the lateral open bite will be less. Second, the bracket positioning is contributing to the problem. Overall this is a beautifully bracketed case-clean and accurate. Good job! However the canine bracket is a little too incisally placed for a case that needs virtually no bite opening. Because of this it is not erupted enough. Reposition the bracket 1.5mm to the gingival and your problem will be solved.
The bite opening in the premolar area occurs because Newton’s 3rd law always works. The opposite reaction to pulling the canine down is an intrusive force on the premolars and lateral incisor. This minor movement will resolve when you use stiffer wires. Settling issues such as these are more easily corrected in light wires as opposed to stiffer rectangular wires as you suggested. The stiff wire will overpower the elastics, rendering them ineffective. That is why many times problems such as these are corrected during finishing. The lighter wire, combined with finishing bends, may be enough to help this case settle. If finishing bends alone don’t solve the problem, use finishing elastics in addition to the finishing wire.
Thanks for taking my call the other day; look at this case and note how his bite is not opened sufficiently; additionally he's popping off lower anterior brackets quite frequently. You suggested to return to 016 stainless steel with curves to open the bite. I did this earlier in the treatment and followed the 016 wire with 020 stainless steel with curves. His bite simply won't open (he appears to have strong musculature). I continued treating him with the 50% overbite. I moved on to rectangular wires, placed composite on the lower 1st molars to open the bite, and began space closure. As I close the space, he is still popping a lot of brackets off. At his most recent visit, I placed composite on the 12yr molars to further open his bite. I also removed the composite off of the 6yr molars. This resulted in a posterior open bite. What should I do? On the phone you recommended I go back to 016S with deep curve to open bite...but somehow I don't think it will work. Is bracket positioning the problem?
Your bracket placement is good- the inciso-(and occluso-) gingival position of the brackets on each individual tooth is consistent. Additionally, your bracketing technique appears to be good because the lack of excess cement around the brackets shows that you are cleaning up well. I would probably have placed my upper 3-3 brackets much more incisal- 2 or 3 mm more incisal than you have them- but I don't know if it's worth repositioning all of them at this point. I guess that if all else (see below) fails, I would reposition.
I don't want the uppers to flare so I would not curve the upper wire. (Remember, intrusive forces create the potential for labial crown rotation.) Keep the curved lower wires in until the overbite is 2mm or less. This will take some time. Also, I would bond more composite on the lower molars to open the bite more. This takes occlusal forces out of the game and bite opening will proceed more quickly. Use deep curve in an 016 stainless steel in for a month followed by moderate curve in 020st steel for a month. If this doesn't completely open the bite, increase the curve in the 020 until it is open. Do no upper space closure until the bite is open- that is until the overbite is 2mm or less. Again, NO space closure until the overbite is corrected (don't cheat-it's tempting).
Do you have double buccal tubes on the lower molar bands? If so you may want to consider an overlay utility wire to intrude lower anteriors. This is very complex stuff so it would require a lot of communication between us. Try the curves 1st and evaluate the overbite in 3months.
I have a question regarding molar band and bracket position; especially the second bicuspid brackets. I often find I have problems when I cement molar bands and bond brackets. After I cement the molar bands, I bond the brackets starting with the central incisors and working towards the second bicuspids. I often see large discrepancies of the wire slot height between the molar band and the second bi bracket slot even though the molar bracket slot is positioned close to the middle of the tooth. This happened when I banded and bonded Sarah's teeth today and I had to remove and recement (more occlusally) the molar bands so they were more even with the second bi bracket slot. I do measure the height of the teeth on the model before bracketing so I know how far to bond from the incisal/occlusal aspect. Do I just need to eyeball the molar band position better? Are there any tips or tricks to minimize the molar to second bicuspid discrepancies?
The most important consideration is to use a molar band that is the correct size. Many clinicians use bands that are too large; this causes the band to slide gingivally resulting in the problem you described. If the correct band size is selected, it is much easier to position the band, and hence the bracket, correctly. They just don't slide too gingivally very often (one exception may be when the upper 1st molars have a large 5th cusp). From a mechanical standpoint this is often deleterious to the case because the molar will over erupt and roll in lingually when the bands are too gingivally positioned. This can result in narrowing of the arches which can lead to a whole host of problems (difficulty in ClassII correction comes to mind).
Fitting bands well requires good spacing. Make sure the spacers have worked. If you are forced to wiggle a band through a tight contact, only a band that is too large will get through the contact point because you need "wiggle space". This will result in the band and therefore the bracket being positioned too gingivally. If you don't have space you can bond 5-5 and replace the spacers and reappoint for band seating.
Many clinicians bond in different ways but I like to bond starting with the upper left 5 then work around the arch. I usually seat bands after bonding is complete. That way the patient is "freshest"-most cooperative and not experiencing a lot of salivary flow- when bonding. Finish the bonding, take a break (this is a good time for some hygiene instruction) then band. After all the brackets are placed it is easier to see if the molar band is positioned correctly because you can compare it to the rest of the brackets.
The bottom line is this: a good fitting molar band will automatically result in correct bracket placement. The only way to fit molar bands correctly is to have good spacing. So make sure those spacers are used properly and a lot of problems will be solved.
When you make an occlusally directed gable bend, is the apex or tip directed occlusally (as in an upside down triangle)? Why can’t I just close the spaces on a rectangular wire to avoid detorquing problems? At what stage of the wire sequence can I start closing anterior diastemas? I have a case where I am using .020 stainless steel wires with rocking chair curve on the lower to open the bite. The patient has upper anterior spacing from 3 to 3 (spaces were present pre-treatment). Can I close these spaces at the same time while I am opening the bite with the .020 SS? What is the best way to close the spaces? Can I also correct midline discrepancies at this stage of the wire sequencing while opening the bite?
If the space is small (3mm or less) I usually close on 020stainless steel. Close larger spaces on rectangular wire. The reason for this is a lot of space closure on round wire may result in detorquing of the upper anterior teeth, which may be unaesthetic. There is much less loss of torque when closing spaces on large (019x025) rectangular wire. Detorquing is always a problem with chain on round wire. Therefore, if the space is too big, closing on rectangular wire is a good idea. For large (greater than 4mm) diastemas, close the space on large rectangular wire until the space remaining is 2mm. Then use .020stainless steel with a gable bend between the centrals. When closing diastemas on round wire, I often place an occlusally directed gable bend (center bend) between the centrals. The apex of the "V" is directed gingivally. This separates the roots and brings the crowns closer together (tips the roots distally and the crowns mesially) which makes the space closure more stable. Root position is very important for long term stability of the space closure. Closing only a couple of millimeters on round wire with chain doesn't significantly affect the torque. Use chain to close spaces (3-3 for small spaces and 6-6 for larger spaces. Use 6-6 to prevent spaces from opening distal to the canines).
If there is spacing, midlines can be aligned at the 020 stage by shifting teeth if the midline shift is only 1 or 2 millimeters. If the spacing and/or midline shift required is more than 2mms, use chain on rectangular wire to make the correction. Again, prevent loss of torque by closing more than 2mm of space on rectangular wire. Use chain for this procedure. If no spacing exists, use some combination of ClassII, ClassIII, and oblique elastics to shift the midline. When doing this, remember to “skew” the archwire (expand the side of the wire in the direction you want the midline to shift).
I repositioned the lower right 2 about 1 mm gingivally to help lock in the occlusion. I used .016 nitinol on the lower and .016 stainless steel on the upper. I want to increase the overbite by 1 to 2mm. Should I reposition the upper anteriors gingivally or can I use a triangular elastic to bring them down? Also, the lower right 6 is tipped lingually. How do I upright this? Will this be corrected once I shift to rectangular wire? Do I still need to use rectangular wire if I don’t need to change the torque of the teeth?
The bite is slightly open because the bicuspid brackets(especially the upper) are a little gingivally positioned, which results in a small amount of bite opening. I wouldn't reposition brackets because the bite will settle and deepen a little after removal. Finishing (step up bends in the lower anterior and step down bends in the upper anterior) combined with finishing elastics on a finishing wire (I like 018 stainless steel) will increase the overbite by 1 to 2mm.
The lower 6 often rolls in (rotates lingually) because the bracket is positioned too gingivally. That causes extrusion and therefore lingual rotation (remember any extrusive force has the potential to create a lingual rotational tendency, or moment). The bracket must be repositioned 2mm towards the occlusal. Either use direct bond a bracket or fit a new band.
After I change the band on the 6, should I use a .016 nitinol or I can go straight to a finishing wire (.018 stainless steel)? How long before this molar uprights? After removal of the braces, will the bite settle if I use both upper and lower full coverage plastic retainers? If no torque change is required, do I need to use rectangular wire?
Reposition the band, go to 016 nitinol for a month, then to finishing wires. The molar will take 6 weeks to upright. If it doesn't upright as a result of bracket repositioning, use rectangular wire (019x025 nitinol is effective)for 6 to 8 weeks. You will need torque control (rectangular wire) in this situation about half of the time. No rectangular wire is necessary if the torque is OK, provided you don’t have to do any mechanics such as Class II correction or space closure. Applying elastics or chain may cause a loss of torque so do these mechanics on rectangular wire, even if the torque is acceptable. Remember, it is far more difficult to reestablish torque than it is to maintain it.
Finishing bends are used to resolve minor settling issues. One of the reasons I like a lower 3-3 lingual bonded retainer is because settling can occur. Essix (clear plastic full coverage)upper and lower retainers don't allow this. Many clinicians make a lower 3-3 Essix to solve this problem. I don’t like these retainers because of their size (they are so small that they don’t seem to fit as well as the full coverage retainers). They are also tough to make. However, the Essix manual does recommend lower 3-3 plastic retainers so it may be something you want to try.
Thursday, November 24, 2011
Diagnosis and treatment of mesially rotated upper 1st molars
Often, a Class II molar relationship develops because the upper 1st molars are mesially rotated. Recent studies show that mesial molar rotation exists in over 80% of Class II malocclusions (1). The importance of molar rotation in the development of Class II occlusion has been recognized for well over a century. In 1906 Angle wrote that the upper 1st molar is the key to development of good occlusion (2). Strang, the author of the 1950 edition of the Textbook of Orthodontics, writes, “Rotation of teeth often appears in the maxillary arch…and the mesio-lingual cusp of the maxillary molar resists displacement so strongly that the crown often rotates bodily around this …root" (3). In the June, 2003 issue of the Angle Orthodontist, authors Gunduz et al. described the etiology of upper molar rotation:
“The space between the buccal and lingual cortical plates becomes narrow anterior to the first-molar roots. When the upper first molar drifts mesially, the large lingual root contacts the lingual plate and allows the two buccal roots to rotate mesio-lingually. The occlusal surface of the first permanent molar is trapezoidal in shape, with the long diagonal from distolingual to mesiobuccal. Therefore, more mesio-distal space is used in the dental arch when this tooth rotates mesially with the lingual root as the axis. By correction of these rotations, one to two mm of arch length per side and partial Class II correction can be achieved. These corrections also are needed to provide good intercuspation."(4)
Ricketts (5) proposed a method of diagnosing mesial rotation of the upper first molar. This method has been widely used for the last 30 years. To determine if mesial rotation exists, view the upper arch from the occlusal and draw a line from the distal buccal through the palatal cusp of the upper molar. That line should pass through the opposite canine.

The figure above shows a correctly rotated molar. The line as described by Ricketts passes through the canine on the opposite side of the arch. Compare that picture to the one below, which shows mesially rotated molars.


Ricketts’ line passes through the opposite bicuspids. The molars are mesially rotated. This results in a Class II molar relationship.


The same patient after molar distal rotation has been accomplished. Ricketts’ line passes through the opposite canine. The molar relationship is Class I.
Why this is important
In normal occlusion, the palatal cusp of the upper 1st molar occludes with the central pit of the lower 1st molar. When the upper molar is mesially rotated, the palatal cusp is in a posterior position. This forces the mandible into a posterior (Class II) position. By distally rotating the molars the palatal cusp is positioned anteriorly. Upper palatal cusp/lower central fossa occlusion encourages forward positioning of the entire mandibular dentition. This results in a more anterior (Class I) mandibular position. Therefore, proper molar rotation results in correction of many Class II malocclusions.
Many clinicians further encourage forward mandibular positioning by expanding the upper arch. The rationale for this is the wider maxilla will accept the mandible in a more forward (Class I) position. Expansion and distal rotation of upper 1st molars has been used to correct Class II malocclusions for over a century. Many appliances can be used to make this correction. Proper manipulation of the inner bow of a headgear has been one of the most often used methodologies. Today, since the use of headgear is declining in most treatment systems, many clinicians simply use arch wires.
There are other advantages to proper upper molar positioning. Correctly rotated molars occupy less space than do molars that are incorrectly rotated. Up to 2 mm of space per side can be gained by correctly rotating the upper molars.

Correct molar rotation (left) and incorrect rotation (right). Notice the amount of space required in each situation.
Bracket position and its effect on molar rotation
Bracket position is critical in the effort to achieve proper upper molar rotation. Whether a band or direct bond bracket is used, the position of the bracket is evaluated by viewing the bracket from the occlusal. If the most anterior portion of the bracket bisects the mesio-buccal cusp, the bracket is placed correctly. When the upper molar band fits well, the bracket is automatically placed in the correct position. Problems arise when a band that is too large is used. The most common reason for using too large a band is insufficient space for band seating. Lack of space is almost always caused by incorrect use of spacers. When the contacts are tight, the clinician is forced to “wiggle” the band through the contacts to seat it. This is impossible to do with a band that is the correct size. Only a band that is too large may be wiggled into place. Bands that are too large result in poor position of the attachment. Poor bracket positioning means that sufficient distal rotation cannot be accomplished with a straight arch wire. To insure sufficient distal rotation, fit the bands correctly. If a bracket is bonded, carefully evaluate the bracket position from the occlusal view. If the bracket is not in the correct position, reposition the band or bonded bracket immediately.
The pictures below show an incorrectly placed band (top) and a correctly placed band (bottom).

Incorrect band size leads to incorrect bracket position. Proper molar position is impossible to attain with a straight wire.

Correct band position leads to correct bracket position. A straight wire results in good molar position.
Archwire bends to achieve distal molar rotation
When a patient presents with severely mesially rotated molars, good bracket position may not be enough to gain proper rotation. Toe-in bends are routinely used to correct severely mesially rotated molars. A 2X4 set-up with 45 degree bends mesial to the molars is an effective molar rotator. This also promotes upper arch expansion, as a toe-in close to the molar not only distally rotates the molar but also expands it by moving the crown buccally. Remember, for these mechanics to be effective, the bend must be an off-center bend. This means that the lateral segments must be bypassed (either left unbracketed or bypassed with a utility arch type bend).

Note: the shaded molar in the picture shows the movement that the 1st molar will experience.
An additional benefit of lateral segment bypass is arch development. This is due to the “Frankel effect”. Frankel appliances, which were developed in East Germany immediately after World War II, correct malocclusions by upsetting muscle balance. They consist of flanges that push muscles away from the arches in an effort to develop the arches(6). For instance a Frankel appliance to correct a Class III occlusion has flanges in the anterior vestibule on the upper arch. These flanges push the upper lip away from the teeth. The created muscular imbalance encourages the arches to develop into the void. The “Frankel effect” has proven to be reliable, especially in young patients. When using an arch wire that bypasses the lateral segments, the wire pushes the cheeks away from the arch. This allows lateral development of the arches into the void created by the wire.
Here is an example of how distal molar rotation is used to achieve a Class I molar relationship:


Pretreatment diagnosis: 4mm Class II as a result of mesially rotated molars


Treatment description:
The phase 1 treatment consisted of a 2X 4 set up in both arches. After leveling and aligning, expansion (using an expanded arch wire) and distal rotation (using bilateral toe-in bends) of the upper molars was accomplished. This corrected the ClassII molar relationship. These arch wires were kept in until the canines and bicuspids erupted. At this point the patient is ready for phase 2, which will consist of simply leveling and aligning, then using Class II elastics if necessary to correct any lingering ClassII relationship.
Because the lateral segments must be bypassed for toe-ins to be effective, this set-up is ideally suited for early treatment. Establishing the correct distal rotation of the upper molars is one of the most important benefits of early treatment. Proper rotation of the upper molars is an essential aspect of a Class I relationship. By establishing the correct molar relationship in the mixed dentition, a child’s growth and development can proceed normally.
In conclusion, proper distal rotation of the upper 1st molar is critical in the development and maintenance of a Class I molar relationship. Mild mesial rotation can be corrected by proper bracket positioning. Severe rotations call for more aggressive intervention. Bypassing the lateral segments and using toe-in bends mesial to the molars aid in the correction of even the most severe rotations. Without proper upper molar position, ideal occlusion is difficult to obtain.
References
1) Mesial rotation of upper first molars in Class II division 1 malocclusion in the mixed dentition: a controlled blind study. Progress in Orthodontics Vol12 issue 2 pp107-113 Nov, 2011.
2) Angle, Edward H.: “The Upper First Molar as a Basis of Diagnosis in Orthodontics.” Items of Interest, Vol. 28, June, 1906.
3) Strang, R.H. : Textbook of Orthodontics, Third Edition, 1950.
4) Gündüz, A. G. Crismani, H. P. Bantleon, Klaus D. Hönigl, and Bjorn U. Zachrisson (2003) An Improved Transpalatal Bar Design. Part II. Clinical Upper Molar Derotation—Case Report. The Angle Orthodontist: June 2003, Vol. 73, No. 3, pp. 244-248.
5) Ricketts RM. Occlusion-the medium of dentistry. J Prosthet Dent 1969; 21:39-60.
6) Prabhu, N. Interception of class II div.1 malocclusion by phase 1 treatment with Frankel appliance. JIADS: Vol 2 Issue 2. April 2011, p62.
“The space between the buccal and lingual cortical plates becomes narrow anterior to the first-molar roots. When the upper first molar drifts mesially, the large lingual root contacts the lingual plate and allows the two buccal roots to rotate mesio-lingually. The occlusal surface of the first permanent molar is trapezoidal in shape, with the long diagonal from distolingual to mesiobuccal. Therefore, more mesio-distal space is used in the dental arch when this tooth rotates mesially with the lingual root as the axis. By correction of these rotations, one to two mm of arch length per side and partial Class II correction can be achieved. These corrections also are needed to provide good intercuspation."(4)
Ricketts (5) proposed a method of diagnosing mesial rotation of the upper first molar. This method has been widely used for the last 30 years. To determine if mesial rotation exists, view the upper arch from the occlusal and draw a line from the distal buccal through the palatal cusp of the upper molar. That line should pass through the opposite canine.

The figure above shows a correctly rotated molar. The line as described by Ricketts passes through the canine on the opposite side of the arch. Compare that picture to the one below, which shows mesially rotated molars.


Ricketts’ line passes through the opposite bicuspids. The molars are mesially rotated. This results in a Class II molar relationship.


The same patient after molar distal rotation has been accomplished. Ricketts’ line passes through the opposite canine. The molar relationship is Class I.
Why this is important
In normal occlusion, the palatal cusp of the upper 1st molar occludes with the central pit of the lower 1st molar. When the upper molar is mesially rotated, the palatal cusp is in a posterior position. This forces the mandible into a posterior (Class II) position. By distally rotating the molars the palatal cusp is positioned anteriorly. Upper palatal cusp/lower central fossa occlusion encourages forward positioning of the entire mandibular dentition. This results in a more anterior (Class I) mandibular position. Therefore, proper molar rotation results in correction of many Class II malocclusions.
Many clinicians further encourage forward mandibular positioning by expanding the upper arch. The rationale for this is the wider maxilla will accept the mandible in a more forward (Class I) position. Expansion and distal rotation of upper 1st molars has been used to correct Class II malocclusions for over a century. Many appliances can be used to make this correction. Proper manipulation of the inner bow of a headgear has been one of the most often used methodologies. Today, since the use of headgear is declining in most treatment systems, many clinicians simply use arch wires.
There are other advantages to proper upper molar positioning. Correctly rotated molars occupy less space than do molars that are incorrectly rotated. Up to 2 mm of space per side can be gained by correctly rotating the upper molars.

Correct molar rotation (left) and incorrect rotation (right). Notice the amount of space required in each situation.
Bracket position and its effect on molar rotation
Bracket position is critical in the effort to achieve proper upper molar rotation. Whether a band or direct bond bracket is used, the position of the bracket is evaluated by viewing the bracket from the occlusal. If the most anterior portion of the bracket bisects the mesio-buccal cusp, the bracket is placed correctly. When the upper molar band fits well, the bracket is automatically placed in the correct position. Problems arise when a band that is too large is used. The most common reason for using too large a band is insufficient space for band seating. Lack of space is almost always caused by incorrect use of spacers. When the contacts are tight, the clinician is forced to “wiggle” the band through the contacts to seat it. This is impossible to do with a band that is the correct size. Only a band that is too large may be wiggled into place. Bands that are too large result in poor position of the attachment. Poor bracket positioning means that sufficient distal rotation cannot be accomplished with a straight arch wire. To insure sufficient distal rotation, fit the bands correctly. If a bracket is bonded, carefully evaluate the bracket position from the occlusal view. If the bracket is not in the correct position, reposition the band or bonded bracket immediately.
The pictures below show an incorrectly placed band (top) and a correctly placed band (bottom).

Incorrect band size leads to incorrect bracket position. Proper molar position is impossible to attain with a straight wire.

Correct band position leads to correct bracket position. A straight wire results in good molar position.
Archwire bends to achieve distal molar rotation
When a patient presents with severely mesially rotated molars, good bracket position may not be enough to gain proper rotation. Toe-in bends are routinely used to correct severely mesially rotated molars. A 2X4 set-up with 45 degree bends mesial to the molars is an effective molar rotator. This also promotes upper arch expansion, as a toe-in close to the molar not only distally rotates the molar but also expands it by moving the crown buccally. Remember, for these mechanics to be effective, the bend must be an off-center bend. This means that the lateral segments must be bypassed (either left unbracketed or bypassed with a utility arch type bend).

Note: the shaded molar in the picture shows the movement that the 1st molar will experience.
An additional benefit of lateral segment bypass is arch development. This is due to the “Frankel effect”. Frankel appliances, which were developed in East Germany immediately after World War II, correct malocclusions by upsetting muscle balance. They consist of flanges that push muscles away from the arches in an effort to develop the arches(6). For instance a Frankel appliance to correct a Class III occlusion has flanges in the anterior vestibule on the upper arch. These flanges push the upper lip away from the teeth. The created muscular imbalance encourages the arches to develop into the void. The “Frankel effect” has proven to be reliable, especially in young patients. When using an arch wire that bypasses the lateral segments, the wire pushes the cheeks away from the arch. This allows lateral development of the arches into the void created by the wire.
Here is an example of how distal molar rotation is used to achieve a Class I molar relationship:


Pretreatment diagnosis: 4mm Class II as a result of mesially rotated molars


Treatment description:
The phase 1 treatment consisted of a 2X 4 set up in both arches. After leveling and aligning, expansion (using an expanded arch wire) and distal rotation (using bilateral toe-in bends) of the upper molars was accomplished. This corrected the ClassII molar relationship. These arch wires were kept in until the canines and bicuspids erupted. At this point the patient is ready for phase 2, which will consist of simply leveling and aligning, then using Class II elastics if necessary to correct any lingering ClassII relationship.
Because the lateral segments must be bypassed for toe-ins to be effective, this set-up is ideally suited for early treatment. Establishing the correct distal rotation of the upper molars is one of the most important benefits of early treatment. Proper rotation of the upper molars is an essential aspect of a Class I relationship. By establishing the correct molar relationship in the mixed dentition, a child’s growth and development can proceed normally.
In conclusion, proper distal rotation of the upper 1st molar is critical in the development and maintenance of a Class I molar relationship. Mild mesial rotation can be corrected by proper bracket positioning. Severe rotations call for more aggressive intervention. Bypassing the lateral segments and using toe-in bends mesial to the molars aid in the correction of even the most severe rotations. Without proper upper molar position, ideal occlusion is difficult to obtain.
References
1) Mesial rotation of upper first molars in Class II division 1 malocclusion in the mixed dentition: a controlled blind study. Progress in Orthodontics Vol12 issue 2 pp107-113 Nov, 2011.
2) Angle, Edward H.: “The Upper First Molar as a Basis of Diagnosis in Orthodontics.” Items of Interest, Vol. 28, June, 1906.
3) Strang, R.H. : Textbook of Orthodontics, Third Edition, 1950.
4) Gündüz, A. G. Crismani, H. P. Bantleon, Klaus D. Hönigl, and Bjorn U. Zachrisson (2003) An Improved Transpalatal Bar Design. Part II. Clinical Upper Molar Derotation—Case Report. The Angle Orthodontist: June 2003, Vol. 73, No. 3, pp. 244-248.
5) Ricketts RM. Occlusion-the medium of dentistry. J Prosthet Dent 1969; 21:39-60.
6) Prabhu, N. Interception of class II div.1 malocclusion by phase 1 treatment with Frankel appliance. JIADS: Vol 2 Issue 2. April 2011, p62.
Sunday, November 20, 2011
Anterior labial root torque
When upper anterior teeth, particularly lateral incisors, are in cross bite, they often need labial root torque. Normally positioned lateral incisor brackets, due to the torque built into those brackets, encourage the expression of lingual root torque. In cases where labial root torque is desired, the laterals never look quite right when normal torque expression occurs. My answer to this problem is to place the lateral incisor brackets on upside down. Flipping the brackets changes the torque expression from predominately lingual root torque to predominately labial root torque when rectangular wire is used.


Flipped upper lateral incisor bracket (top)
Normally positioned upper lateral incisor bracket (bottom)
The procedure to encourage labial root torque is as follows:
1) Create space in the arch form for the blocked out lateral incisor. This can be done on the initial arch wire by packing open coil spring between the central and canine in non-extraction cases, or by using a combination of coils and/or lacebacks in extraction cases. Remember not to pack too much coil on the initial arch wire (my coil springs are usually about 2mm longer than the space between the brackets on the adjacent teeth). This helps prevent distortion of the arch form. Be patient; use a slightly larger (about 2mm) piece of coil each month until enough space in the arch form is created to accommodate the blocked out tooth.


Blocked out upper right lateral.
Labial root torque will be needed.


Creating space with lacebacks and coil spring.
2) Once sufficient space is created, bracket the blocked out tooth (in our example, the upper lateral incisor). Place the bracket on upside down and engage the tooth. A light flexible arch wire must be used because that wire must be deflected a significant amount to engage the tooth. Often, as in the case shown here, a tandem arch wire set up is used. Additionally, in patients with deep bites, the bracket on the blocked out tooth may cause severe occlusal interferences. If this is the case, temporarily prop the bite open by bonding composite to the occlusal surface of both lower 1st molars. Remove the composite after the crossbite is corrected.


The lateral can be moved into the arch form after space is created. Note how composite is used to temporarily eliminate the occlusal interferences.
3) This set-up will result in labial movement of the crown. Because round wire is being used, no torque expression occurs as a result of torque in the bracket slot. At this stage of treatment it doesn't matter what the torque in the bracket slot is. Once the crossbite is corrected, remove the composite from the occlusal surface of the lower molars. The overbite will help retain the labial crown movement.

Crown is now in place. Note the need for labial root torque.
4)Once initial aligning is complete, begin torque expression by using a low load deflection rectangular arch wire. I often use 019x025 heat activated nickel titanium (HANT) followed by 021x025 HANT. Filling the slot encourages the expression of torque. The upside down bracket means the torque in the bracket slot encourages labial root/lingual crown torque. Because of anterior overbite, occlusion helps the crown retain its position while labial root torque occurs. Usually about 10 weeks of 021x025 HANT is necessary to achieve full torque expression. Leave the bracket on upside down for the whole treatment. That way correct torque expression is encouraged throughout the whole treatment.


Rectangular wire (021x025HANT) fills the slot. Note expression of labial root torque.
The treatment photos below (courtesy of Dr. Gerald Samson) demonstrate how much improvement in root position is possible with this technique.




Flipped upper lateral incisor bracket (top)
Normally positioned upper lateral incisor bracket (bottom)
The procedure to encourage labial root torque is as follows:
1) Create space in the arch form for the blocked out lateral incisor. This can be done on the initial arch wire by packing open coil spring between the central and canine in non-extraction cases, or by using a combination of coils and/or lacebacks in extraction cases. Remember not to pack too much coil on the initial arch wire (my coil springs are usually about 2mm longer than the space between the brackets on the adjacent teeth). This helps prevent distortion of the arch form. Be patient; use a slightly larger (about 2mm) piece of coil each month until enough space in the arch form is created to accommodate the blocked out tooth.


Blocked out upper right lateral.
Labial root torque will be needed.


Creating space with lacebacks and coil spring.
2) Once sufficient space is created, bracket the blocked out tooth (in our example, the upper lateral incisor). Place the bracket on upside down and engage the tooth. A light flexible arch wire must be used because that wire must be deflected a significant amount to engage the tooth. Often, as in the case shown here, a tandem arch wire set up is used. Additionally, in patients with deep bites, the bracket on the blocked out tooth may cause severe occlusal interferences. If this is the case, temporarily prop the bite open by bonding composite to the occlusal surface of both lower 1st molars. Remove the composite after the crossbite is corrected.


The lateral can be moved into the arch form after space is created. Note how composite is used to temporarily eliminate the occlusal interferences.
3) This set-up will result in labial movement of the crown. Because round wire is being used, no torque expression occurs as a result of torque in the bracket slot. At this stage of treatment it doesn't matter what the torque in the bracket slot is. Once the crossbite is corrected, remove the composite from the occlusal surface of the lower molars. The overbite will help retain the labial crown movement.

Crown is now in place. Note the need for labial root torque.
4)Once initial aligning is complete, begin torque expression by using a low load deflection rectangular arch wire. I often use 019x025 heat activated nickel titanium (HANT) followed by 021x025 HANT. Filling the slot encourages the expression of torque. The upside down bracket means the torque in the bracket slot encourages labial root/lingual crown torque. Because of anterior overbite, occlusion helps the crown retain its position while labial root torque occurs. Usually about 10 weeks of 021x025 HANT is necessary to achieve full torque expression. Leave the bracket on upside down for the whole treatment. That way correct torque expression is encouraged throughout the whole treatment.


Rectangular wire (021x025HANT) fills the slot. Note expression of labial root torque.
The treatment photos below (courtesy of Dr. Gerald Samson) demonstrate how much improvement in root position is possible with this technique.


Thursday, May 5, 2011
More questions and answers
Question: Why are Class III cases with open bite tendencies so difficult for beginners to treat?
Class III open bites are difficult for anyone, not just beginners. In these cases you have two problems that are tough to control. With Class III’s, you are at the mercy of mandibular growth. This growth accelerates during the growth spurt which means the Class III often worsens. In other words growth works against your treatment. Often Class III elastics are effective in correcting mild to moderate Class III problems. However, any inter-arch mechanics (in high angled patients, because muscle strength in these patients is usually not strong enough to resist the vertical component of force resulting from these mechanics) can make the high angled problem worse. Since virtually every published study involving facial aesthetics show that excessive face height leads to the most unattractive faces, it is important to minimize increases in face height in patients who already have long faces.
In these cases, extractions are sometimes effective. Extractions and space closure are effective in limiting increases in the vertical dimension and in many cases can actually reduce the anterior facial height. However, as this happens, the mandible rotates into a more closed position and, because the mandible opens and closes on an arc, it also moves forward, which worsens the Class III. So you see, most of what you can do in these cases have consequences that worsen other aspects of the malocclusion. There are no easy answers. This is why they are so difficult.
Question: One of my patients has a deep bite and bad oral hygiene. Every month he comes in, brackets are missing. Is it the bracket positioning that is responsible for the bonding failures? What do you suggest?
The bracket positioning is the least of your worries. Orthodontic bonding failures occur more in poor cooperators than in good cooperators. Poor cooperation is the major problem. My advice: either the patient improves his oral hygiene or you remove the braces. Don't tolerate this stuff. The patient and family are not upholding their end of the contract. The worst thing that can happen in an orthodontic case is decalcification due to bad hygiene. This problem will make any malocclusion look mild in comparison. Don't allow the possibility of decalcification to rear its ugly head. It's either clean teeth or no braces. It is just that simple. Do not compromise.
Question: I am a little confused about the shaping of arch wires. Is the upper wire 3mm longer than lower? What arch wire shape do you usually buy? There are so many sizes (for example wide, narrow, natural) that I am not sure which ones should I buy. Should I use the same arch form for nitinol wires as I do for stainless steel wires?
When coordinating arch wires, it is the width of the wire we are altering. The length simply depends on the total amount of wire needed to engage all the brackets. We have no control over this as it just depends on the total arch length. When buying wire, buy upper and lower broad arch forms for both stainless steel and nitinol. The original arch form of the stainless steel wire is less important than nitinol, because you will be shaping all stainless steel wires based on the pre-treatment arch form. Since the more flimsy (scientific term: low load-deflection rate) nitinol wire does not, due to its lack of stiffness, affect arch width as much as stiffer (high load deflection rate) wires like stainless steel, we do not routinely reshape nitinol wire (because of its flexibility it is hard to do anyway) and simply use the broad arch form in both the upper and lower arches.
Question: Do you prefer to use standard size brackets or minis?
I actually like the standard size brackets. Larger (wider) brackets result in better rotation control. Additionally, standard brackets have more surface area on the bonding pad which results in greater bond strength. Many doctors prefer the mini brackets because they are more aesthetic, but I don’t think the aesthetics of mini stainless steel brackets are that much different than the standard sized brackets.
Question: In extraction cases, what teeth do you usually extract?
If there is minimal lower arch crowding with a Class II tendency, I tend to extract upper 4’s and lower 5's. In this situation, reciprocal space closure results in more forward lower molar movement than forward upper molar movement. This moves the molars closer to a Class I relationship. In cases that are close to a full cusp Class II with minimal lower arch crowding, I often extract only upper 1st bicuspids and finish the case with Class II molars. If the case is Class I and extractions are necessary, four 1st bicuspid extractions is usually my treatment of choice.
Question: I am starting a case that has anterior spacing in both the upper and lower arches. How are these cases best started? Should I use 6-6 chain right from the start in 016 Niti wire? Or do I wait until later in the wire sequence?
For a case with spacing, it is usually prudent to progress into stiffer wires before initiating space closure. Always get the bite open to the desired level before initiating space closure. Additionally, you want the teeth to be sliding on a rigid arch wire so side effects of space closure are minimal. If the wire is too flimsy the chain can collapse the lateral segments, which results in a lot of tipping that you may not want. So wait to begin space closure. When you finally start space closure, if you want to reduce anterior torque, use round wire (020ss is my choice) when you close the spaces. If maintaining torque is a concern, wait until you are in 019X025 stainless steel (rectangular wire) before initiating space closure. The advantage of space closure on rectangular wire is the amount of control it provides but, because of the friction created due to the relatively full slot (there is not a lot of “slop” with 019X025 wire in an 022 slot), space closure may be inhibited. This is frustrating. Frictional forces are much less when closing space on 020 stainless steel, but this advantage is offset by the disadvantage of lack of control that is a result of the wire not filling the slot to a significant degree.
Many practitioners prefer to close space on round wire due to ease of space closure. For me, it depends on the torque of the anterior teeth. If torque is excessive, round is OK. If not, be careful. It is not easy to regain lost torque. Also, de-torqued anterior teeth (as the teeth de-torque the incisal edges rotate lingually) are often esthetically and functionally inferior to properly torqued teeth.
Question: I am treating a 10 year old boy with a 2x4 set-up on both upper and lower arches. His pretreatment overbite was 8mm. I'm intruding lower anterior teeth with a tip back set-up. Should I also intrude the upper anteriors?
It depends. My decision to intrude the upper anterior teeth is based on the amount of gingival display. If he has a smile that is too gummy, use tip back bends to intrude the upper anteriors. If his smile line is OK, just intrude the lowers.
Class III open bites are difficult for anyone, not just beginners. In these cases you have two problems that are tough to control. With Class III’s, you are at the mercy of mandibular growth. This growth accelerates during the growth spurt which means the Class III often worsens. In other words growth works against your treatment. Often Class III elastics are effective in correcting mild to moderate Class III problems. However, any inter-arch mechanics (in high angled patients, because muscle strength in these patients is usually not strong enough to resist the vertical component of force resulting from these mechanics) can make the high angled problem worse. Since virtually every published study involving facial aesthetics show that excessive face height leads to the most unattractive faces, it is important to minimize increases in face height in patients who already have long faces.
In these cases, extractions are sometimes effective. Extractions and space closure are effective in limiting increases in the vertical dimension and in many cases can actually reduce the anterior facial height. However, as this happens, the mandible rotates into a more closed position and, because the mandible opens and closes on an arc, it also moves forward, which worsens the Class III. So you see, most of what you can do in these cases have consequences that worsen other aspects of the malocclusion. There are no easy answers. This is why they are so difficult.
Question: One of my patients has a deep bite and bad oral hygiene. Every month he comes in, brackets are missing. Is it the bracket positioning that is responsible for the bonding failures? What do you suggest?
The bracket positioning is the least of your worries. Orthodontic bonding failures occur more in poor cooperators than in good cooperators. Poor cooperation is the major problem. My advice: either the patient improves his oral hygiene or you remove the braces. Don't tolerate this stuff. The patient and family are not upholding their end of the contract. The worst thing that can happen in an orthodontic case is decalcification due to bad hygiene. This problem will make any malocclusion look mild in comparison. Don't allow the possibility of decalcification to rear its ugly head. It's either clean teeth or no braces. It is just that simple. Do not compromise.
Question: I am a little confused about the shaping of arch wires. Is the upper wire 3mm longer than lower? What arch wire shape do you usually buy? There are so many sizes (for example wide, narrow, natural) that I am not sure which ones should I buy. Should I use the same arch form for nitinol wires as I do for stainless steel wires?
When coordinating arch wires, it is the width of the wire we are altering. The length simply depends on the total amount of wire needed to engage all the brackets. We have no control over this as it just depends on the total arch length. When buying wire, buy upper and lower broad arch forms for both stainless steel and nitinol. The original arch form of the stainless steel wire is less important than nitinol, because you will be shaping all stainless steel wires based on the pre-treatment arch form. Since the more flimsy (scientific term: low load-deflection rate) nitinol wire does not, due to its lack of stiffness, affect arch width as much as stiffer (high load deflection rate) wires like stainless steel, we do not routinely reshape nitinol wire (because of its flexibility it is hard to do anyway) and simply use the broad arch form in both the upper and lower arches.
Question: Do you prefer to use standard size brackets or minis?
I actually like the standard size brackets. Larger (wider) brackets result in better rotation control. Additionally, standard brackets have more surface area on the bonding pad which results in greater bond strength. Many doctors prefer the mini brackets because they are more aesthetic, but I don’t think the aesthetics of mini stainless steel brackets are that much different than the standard sized brackets.
Question: In extraction cases, what teeth do you usually extract?
If there is minimal lower arch crowding with a Class II tendency, I tend to extract upper 4’s and lower 5's. In this situation, reciprocal space closure results in more forward lower molar movement than forward upper molar movement. This moves the molars closer to a Class I relationship. In cases that are close to a full cusp Class II with minimal lower arch crowding, I often extract only upper 1st bicuspids and finish the case with Class II molars. If the case is Class I and extractions are necessary, four 1st bicuspid extractions is usually my treatment of choice.
Question: I am starting a case that has anterior spacing in both the upper and lower arches. How are these cases best started? Should I use 6-6 chain right from the start in 016 Niti wire? Or do I wait until later in the wire sequence?
For a case with spacing, it is usually prudent to progress into stiffer wires before initiating space closure. Always get the bite open to the desired level before initiating space closure. Additionally, you want the teeth to be sliding on a rigid arch wire so side effects of space closure are minimal. If the wire is too flimsy the chain can collapse the lateral segments, which results in a lot of tipping that you may not want. So wait to begin space closure. When you finally start space closure, if you want to reduce anterior torque, use round wire (020ss is my choice) when you close the spaces. If maintaining torque is a concern, wait until you are in 019X025 stainless steel (rectangular wire) before initiating space closure. The advantage of space closure on rectangular wire is the amount of control it provides but, because of the friction created due to the relatively full slot (there is not a lot of “slop” with 019X025 wire in an 022 slot), space closure may be inhibited. This is frustrating. Frictional forces are much less when closing space on 020 stainless steel, but this advantage is offset by the disadvantage of lack of control that is a result of the wire not filling the slot to a significant degree.
Many practitioners prefer to close space on round wire due to ease of space closure. For me, it depends on the torque of the anterior teeth. If torque is excessive, round is OK. If not, be careful. It is not easy to regain lost torque. Also, de-torqued anterior teeth (as the teeth de-torque the incisal edges rotate lingually) are often esthetically and functionally inferior to properly torqued teeth.
Question: I am treating a 10 year old boy with a 2x4 set-up on both upper and lower arches. His pretreatment overbite was 8mm. I'm intruding lower anterior teeth with a tip back set-up. Should I also intrude the upper anteriors?
It depends. My decision to intrude the upper anterior teeth is based on the amount of gingival display. If he has a smile that is too gummy, use tip back bends to intrude the upper anteriors. If his smile line is OK, just intrude the lowers.
Thursday, November 18, 2010
I posted a couple of items from "Practical Reviews in Orthodontics" which is a subscription service that I strongly recommend.It can be found here:
http://www.practicalreviews.com/Orthodontics/Journals/Practical-Reviews-in-Orthodontics-3105.aspx
Here is the description of the service (taken from the practical reviews website):
With the literally thousands of articles published annually in orthodontics, it is virtually an impossible task to sort through and read everything necessary to stay current. And there's the daunting task to even identify all the key clinical developments that are reported on in the numerous journals.
The physician-editors with Practical Reviews in Orthodontics sort through dozens of publications, find the most relevant studies, summarize them, and suggest ways to apply this information in practice. Most of the reviews are available to you in convenient audio format — allowing you to download this material to your laptop, MP3 player or almost any portable device.
Note: none of the material in this post was written by me. This post is taken directly from Practical Reviews. Hopefully, I have given the authors full credit.
An Evaluation of Clinicians' Choices When Selecting Archwires.
McNamara C, Drage KJ, et al: Eur J Orthod; 2010;32 (February): 54-59
Background: Many studies have looked at the stability of orthodontic results. In particular, attention has been paid to the form of the arch. Previous studies have found that using an arch form that maintains intercanine width, intermolar width, and arch length contributes to a stable result.
Objective: To determine the choices clinicians make when choosing arch wires during initial alignment and space closure.
Design: Survey.
Participants: 100 orthodontic practitioners within the Bristol Dental Hospital or who were contacted at local meetings were included in the survey. These consisted of consultant orthodontists (n=37), specialist practitioners (n=36), senior specialist registrars in orthodontics (n=10), and dentists with a special interest in orthodontics (n=17).
Methods: A questionnaire survey was distributed between November 2005 and March 2006. The questionnaire was divided into 2 parts, wires for initial alignment and wires for space closure in a Class I premolar extraction case. For initial alignment wires, clinicians were asked about arch-wire material, dimensions, trade name, arch form, and the importance of these factors when choosing a wire. For the space closure wires, clinicians were asked about arch-wire material, dimensions, use of study models for adaptation, use of symmetry charts, and the importance of these factors when using a wire.
Results: The 100 questionnaires returned represented a 92.6% response rate. A 0.022-inch slot was used by 99% of clinicians. For initial alignment wires, 1 clinician used 0.014 inch multi-stranded stainless steel, while the other 99% used nickel-titanium; of the 99%, 23 used classic NiTi (martensitic stable), 34 used super-elastic (austenitic active), and 34 used heat-activated (martensitic active) NiTi; 9 did not know what type of NiTi they used.
At this stage, arch form was found to be important by 16% of clinicians and the arch width by 23%.For space closure wires, 1 clinician used 0.018- x 0.025-inch NiTi, and the other 99% used stainless steel. All but 5 clinicians felt that adaptation to the canines was important, but there was great diversity on the other landmarks (incisors, premolars, or molars). In addition, the use of casts and symmetry charts varied.
Conclusions: A majority of clinicians felt that preserving a patient's pretreatment arch form was important in the later stages of treatment, but not for selection of initial alignment wires. No uniformity was found in the method used to preserve arch form.
Reviewer's Comments: Although this was not a scientific study of arch form or the ability to maintain arch form, it was interesting that most clinicians at least claimed to be concerned about preservation the lower arch intercanine width. Most of the clinicians rightly believed that arch form selection was less important for early alignment wires when tooth-to-tooth discrepancies override overall arch form characteristics. It would be interesting to look at actual treatment outcomes from this group of practitioners to see if the varied methods used during later treatment stages were equally successful in maintaining the lower arch form.(Reviewer–Brent E. Larson, DDS, MS).
Long-Term Effects of Rapid Maxillary Expansion Followed by Fixed Appliances.
Gurel HG, Memili B, et al: Angle Orthod; 2010;80 (January): 5-9
Background: Maxillary expansion is a routine procedure performed to correct narrow maxillary arch width and posterior cross-bite. We assume, as orthodontists, that our expansion will be stable long term, but is that assumption correct?
Objective: To evaluate the long-term changes in maxillary dental arch widths in patients who were treated with rapid maxillary expansion (RME) appliances followed by edgewise appliances.
Design: This was a retrospective analysis of the records of 41 patients who had been treated for maxillary constriction.
Methods: Maxillary dental casts were available at 4 time periods: before treatment, after maxillary expansion, after complete nonextraction orthodontic therapy, and approximately 5 years later. The maxillary intercanine, interpremolar, and intermolar widths were measured at all 4 intervals. These widths were then compared over time.
Results: The maxillary intermolar, interpremolar, and intercanine widths all increased during palatal expansion treatment. During the time of full-banded, edgewise orthodontic therapy, the intermolar, interpremolar, and intercanine widths decreased. After appliance removal, these widths continued to decrease, with the greatest decrease occurring in the intercanine width, which nearly reached its original pretreatment distance.
Conclusions:
A significant amount of relapse occurs after RME during a second phase of orthodontics, as well as long term.
Reviewer's Comments: I found the information in this study to be useful. I have had similar experiences in patients I have treated using RME followed by routine orthodontics. Long term, these arch widths tend to decrease with time. I believe it is probably due to the stretching of the palatal gingiva, which simply does not accommodate to these greater widths in all patients. It is good to be aware of this information before correction of posterior cross-bites and to consider long-term retention for patients who have been treated for significant palatal constriction.(Reviewer–Vincent G. Kokich, DDS, MSD).
Alignment Efficiency of Damon3 Self-Ligating and Conventional Orthodontic Bracket Systems: A Randomized Clinical Trial.
Scott P, DiBiase A, et al: Am J Orthod Dentofacial Orthop; 2008;134 (October): 470.e1-470.e8
Background: Self-ligating brackets have become increasingly popular. It has been suggested that the Damon3 self-ligating bracket encourages more rapid tooth alignment. In deciding to choose a bracket system, it is important to know if this is true.
Objective/Design: The purpose of this randomized, clinical trial was to compare the clinical efficiency of Damon3 self-ligating brackets with a conventional ligated bracket system during orthodontic tooth alignment.
Participants: The sample for this study consisted of 60 subjects (28 using Synthesis traditional brackets and 32 using Damon3 brackets). All subjects had a mandibular incisor irregularity of 5 to 12 mm, extraction of mandibular first premolars, and the absence of a complete overbite.
Interventions: The same series of initial arch wires ranging from a 0.014-in copper nickel titanium to a 0.019 x 0.025-in stainless steel arch wire were used for each group. Study casts were taken at the start of treatment, at the first arch wire change, and at placement of the final 0.019 x 0.025-in stainless steel arch wire. Little's Irregularity Index was used to measure changes in mandibular incisor alignment.
Results: No significant difference was noted in the initial rate of alignment for either bracket system. The influence of sex, age, and appliance type was statistically insignificant; however, the initial irregularity influenced the rate of tooth movement for both systems with greater irregularity related to more efficient tooth movement.
Conclusions:
Damon3 self-ligating brackets are no more efficient than conventionally ligated preadjusted brackets during tooth alignment.
Reviewer's Comments: Based on claims I have heard, I would have suspected that the Damon3 system would have been more efficient for mandibular incisor alignment. However, once again, it does not surprise me that commonly held orthodontic claims or theories are found to have no basis when exposed to objective research. There may be several good reasons to use the Damon3 self-ligating bracket system, such as reduced staff time in changing arch wires, but the rate of tooth movement is not one of them. (Reviewer–John S. Casko, DDS, MS, PhD).
http://www.practicalreviews.com/Orthodontics/Journals/Practical-Reviews-in-Orthodontics-3105.aspx
Here is the description of the service (taken from the practical reviews website):
With the literally thousands of articles published annually in orthodontics, it is virtually an impossible task to sort through and read everything necessary to stay current. And there's the daunting task to even identify all the key clinical developments that are reported on in the numerous journals.
The physician-editors with Practical Reviews in Orthodontics sort through dozens of publications, find the most relevant studies, summarize them, and suggest ways to apply this information in practice. Most of the reviews are available to you in convenient audio format — allowing you to download this material to your laptop, MP3 player or almost any portable device.
Note: none of the material in this post was written by me. This post is taken directly from Practical Reviews. Hopefully, I have given the authors full credit.
An Evaluation of Clinicians' Choices When Selecting Archwires.
McNamara C, Drage KJ, et al: Eur J Orthod; 2010;32 (February): 54-59
Background: Many studies have looked at the stability of orthodontic results. In particular, attention has been paid to the form of the arch. Previous studies have found that using an arch form that maintains intercanine width, intermolar width, and arch length contributes to a stable result.
Objective: To determine the choices clinicians make when choosing arch wires during initial alignment and space closure.
Design: Survey.
Participants: 100 orthodontic practitioners within the Bristol Dental Hospital or who were contacted at local meetings were included in the survey. These consisted of consultant orthodontists (n=37), specialist practitioners (n=36), senior specialist registrars in orthodontics (n=10), and dentists with a special interest in orthodontics (n=17).
Methods: A questionnaire survey was distributed between November 2005 and March 2006. The questionnaire was divided into 2 parts, wires for initial alignment and wires for space closure in a Class I premolar extraction case. For initial alignment wires, clinicians were asked about arch-wire material, dimensions, trade name, arch form, and the importance of these factors when choosing a wire. For the space closure wires, clinicians were asked about arch-wire material, dimensions, use of study models for adaptation, use of symmetry charts, and the importance of these factors when using a wire.
Results: The 100 questionnaires returned represented a 92.6% response rate. A 0.022-inch slot was used by 99% of clinicians. For initial alignment wires, 1 clinician used 0.014 inch multi-stranded stainless steel, while the other 99% used nickel-titanium; of the 99%, 23 used classic NiTi (martensitic stable), 34 used super-elastic (austenitic active), and 34 used heat-activated (martensitic active) NiTi; 9 did not know what type of NiTi they used.
At this stage, arch form was found to be important by 16% of clinicians and the arch width by 23%.For space closure wires, 1 clinician used 0.018- x 0.025-inch NiTi, and the other 99% used stainless steel. All but 5 clinicians felt that adaptation to the canines was important, but there was great diversity on the other landmarks (incisors, premolars, or molars). In addition, the use of casts and symmetry charts varied.
Conclusions: A majority of clinicians felt that preserving a patient's pretreatment arch form was important in the later stages of treatment, but not for selection of initial alignment wires. No uniformity was found in the method used to preserve arch form.
Reviewer's Comments: Although this was not a scientific study of arch form or the ability to maintain arch form, it was interesting that most clinicians at least claimed to be concerned about preservation the lower arch intercanine width. Most of the clinicians rightly believed that arch form selection was less important for early alignment wires when tooth-to-tooth discrepancies override overall arch form characteristics. It would be interesting to look at actual treatment outcomes from this group of practitioners to see if the varied methods used during later treatment stages were equally successful in maintaining the lower arch form.(Reviewer–Brent E. Larson, DDS, MS).
Long-Term Effects of Rapid Maxillary Expansion Followed by Fixed Appliances.
Gurel HG, Memili B, et al: Angle Orthod; 2010;80 (January): 5-9
Background: Maxillary expansion is a routine procedure performed to correct narrow maxillary arch width and posterior cross-bite. We assume, as orthodontists, that our expansion will be stable long term, but is that assumption correct?
Objective: To evaluate the long-term changes in maxillary dental arch widths in patients who were treated with rapid maxillary expansion (RME) appliances followed by edgewise appliances.
Design: This was a retrospective analysis of the records of 41 patients who had been treated for maxillary constriction.
Methods: Maxillary dental casts were available at 4 time periods: before treatment, after maxillary expansion, after complete nonextraction orthodontic therapy, and approximately 5 years later. The maxillary intercanine, interpremolar, and intermolar widths were measured at all 4 intervals. These widths were then compared over time.
Results: The maxillary intermolar, interpremolar, and intercanine widths all increased during palatal expansion treatment. During the time of full-banded, edgewise orthodontic therapy, the intermolar, interpremolar, and intercanine widths decreased. After appliance removal, these widths continued to decrease, with the greatest decrease occurring in the intercanine width, which nearly reached its original pretreatment distance.
Conclusions:
A significant amount of relapse occurs after RME during a second phase of orthodontics, as well as long term.
Reviewer's Comments: I found the information in this study to be useful. I have had similar experiences in patients I have treated using RME followed by routine orthodontics. Long term, these arch widths tend to decrease with time. I believe it is probably due to the stretching of the palatal gingiva, which simply does not accommodate to these greater widths in all patients. It is good to be aware of this information before correction of posterior cross-bites and to consider long-term retention for patients who have been treated for significant palatal constriction.(Reviewer–Vincent G. Kokich, DDS, MSD).
Alignment Efficiency of Damon3 Self-Ligating and Conventional Orthodontic Bracket Systems: A Randomized Clinical Trial.
Scott P, DiBiase A, et al: Am J Orthod Dentofacial Orthop; 2008;134 (October): 470.e1-470.e8
Background: Self-ligating brackets have become increasingly popular. It has been suggested that the Damon3 self-ligating bracket encourages more rapid tooth alignment. In deciding to choose a bracket system, it is important to know if this is true.
Objective/Design: The purpose of this randomized, clinical trial was to compare the clinical efficiency of Damon3 self-ligating brackets with a conventional ligated bracket system during orthodontic tooth alignment.
Participants: The sample for this study consisted of 60 subjects (28 using Synthesis traditional brackets and 32 using Damon3 brackets). All subjects had a mandibular incisor irregularity of 5 to 12 mm, extraction of mandibular first premolars, and the absence of a complete overbite.
Interventions: The same series of initial arch wires ranging from a 0.014-in copper nickel titanium to a 0.019 x 0.025-in stainless steel arch wire were used for each group. Study casts were taken at the start of treatment, at the first arch wire change, and at placement of the final 0.019 x 0.025-in stainless steel arch wire. Little's Irregularity Index was used to measure changes in mandibular incisor alignment.
Results: No significant difference was noted in the initial rate of alignment for either bracket system. The influence of sex, age, and appliance type was statistically insignificant; however, the initial irregularity influenced the rate of tooth movement for both systems with greater irregularity related to more efficient tooth movement.
Conclusions:
Damon3 self-ligating brackets are no more efficient than conventionally ligated preadjusted brackets during tooth alignment.
Reviewer's Comments: Based on claims I have heard, I would have suspected that the Damon3 system would have been more efficient for mandibular incisor alignment. However, once again, it does not surprise me that commonly held orthodontic claims or theories are found to have no basis when exposed to objective research. There may be several good reasons to use the Damon3 self-ligating bracket system, such as reduced staff time in changing arch wires, but the rate of tooth movement is not one of them. (Reviewer–John S. Casko, DDS, MS, PhD).
Subscribe to:
Comments (Atom)